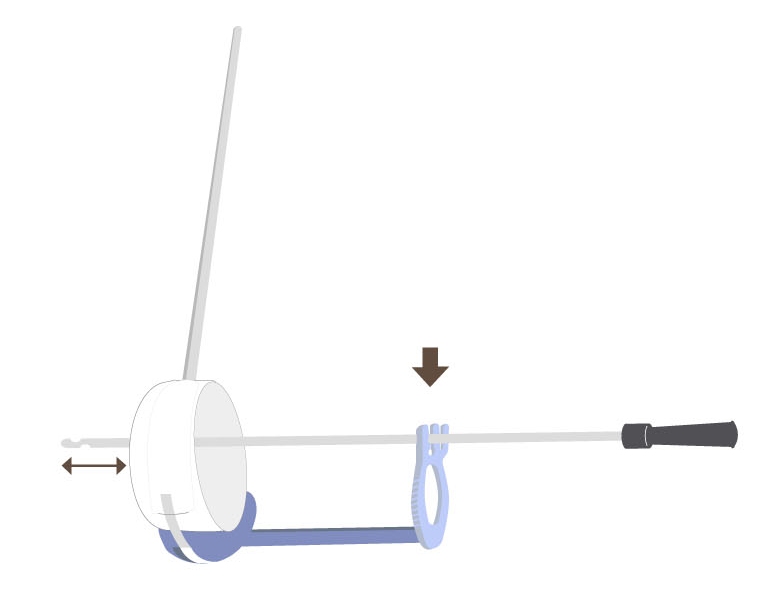
Catheter clamp
with an aperture to fit a 6-Fr catheter.
Padded ring
tractioning the band constricts the ring and applies externa compression.
V-section
to section the band and release the ring compression
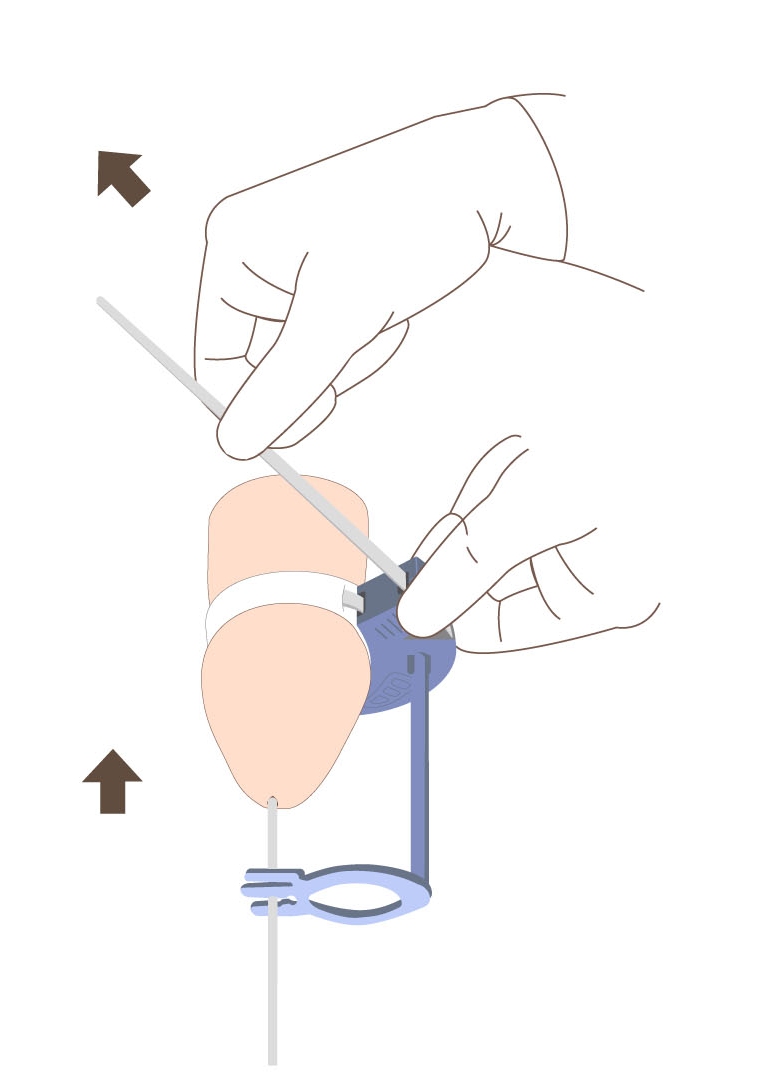
Catheter clamp
with an aperture
to fit a 6-Fr catheter.
to fit a 6-Fr catheter.
Padded ring
tractioning the band
constricts the ring
constricts the ring
and applies external
compression.
compression.
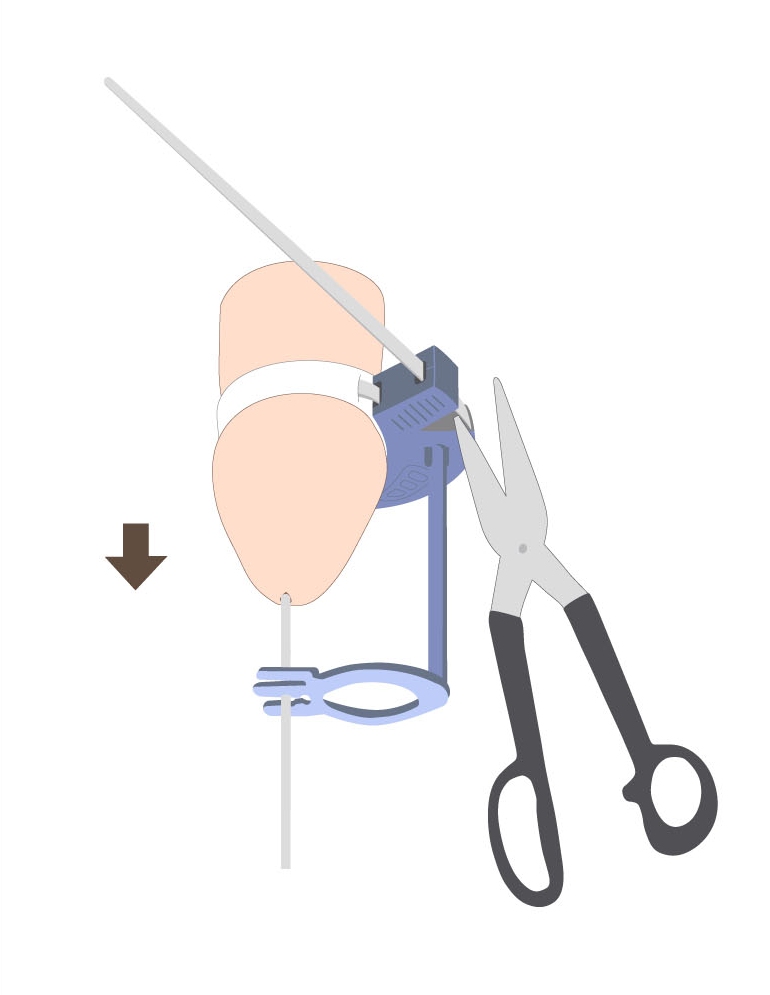
V-section
to section the band
and release
the ring compression
Catheter clamp
with an aperture to fit a 6-Fr catheter.
Padded ring
tractioning the band constricts the ring
and applies external compression.
V-section
to section the band and release the ring compression